Blue Circle
Medi Services

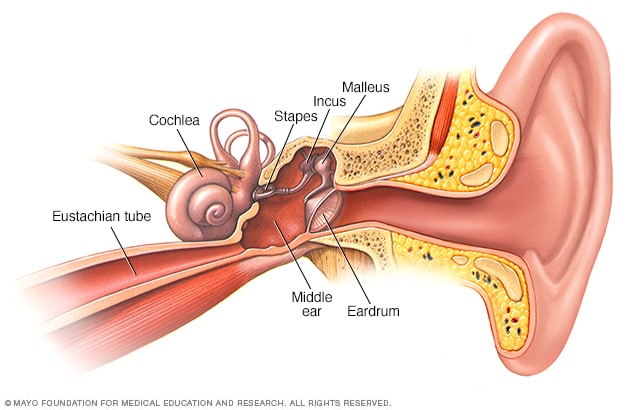
An ear infection (acute otitis media) is most often a bacterial or viral infection that affects the middle ear, the air-filled space behind the eardrum that contains the tiny vibrating bones of the ear. Children are more likely than adults to get ear infections.
Ear infections frequently are painful because of inflammation and buildup of fluids in the middle ear.
Because ear infections often clear up on their own, treatment may begin with managing pain and monitoring the problem. Ear infection in infants and severe cases in general often require antibiotic medications. Long-term problems related to ear infections — persistent fluids in the middle ear, persistent infections or frequent infections — can cause hearing problems and other serious complications.
The onset of signs and symptoms of ear infection is usually rapid.
Signs and symptoms common in children include:
Common signs and symptoms in adults include:
Signs and symptoms of an ear infection can indicate a number of conditions. It's important to get an accurate diagnosis and prompt treatment. Call your child's doctor if:
An adult with ear pain or discharge should see a doctor as soon as possible.
An ear infection is caused by a bacterium or virus in the middle ear. This infection often results from another illness — cold, flu or allergy — that causes congestion and swelling of the nasal passages, throat and eustachian tubes.
The eustachian tubes are a pair of narrow tubes that run from each middle ear to high in the back of the throat, behind the nasal passages. The throat end of the tubes open and close to:
Swelling, inflammation and mucus in the eustachian tubes from an upper respiratory infection or allergy can block them, causing the accumulation of fluids in the middle ear. A bacterial or viral infection of this fluid is usually what produces the symptoms of an ear infection.
Ear infections are more common in children, in part, because their eustachian tubes are narrower and more horizontal — factors that make them more difficult to drain and more likely to get clogged.
Adenoids are two small pads of tissues high in the back of the nose believed to play a role in immune system activity. This function may make them particularly vulnerable to infection, inflammation and swelling.
Because adenoids are near the opening of the eustachian tubes, inflammation or enlargement of the adenoids may block the tubes, thereby contributing to middle ear infection. Inflammation of adenoids is more likely to play a role in ear infections in children because children have relatively larger adenoids.
Conditions of the middle ear that may be related to an ear infection or result in similar middle ear problems include the following:

Risk factors for ear infections include:
Most ear infections don't cause long-term complications. Frequent or persistent infections and persistent fluid buildup can result in some serious complications:
An instrument called a pneumatic otoscope is often the only specialized tool a doctor needs to make a diagnosis of an ear infection. This instrument enables the doctor to look in the ear and judge whether there is fluid behind the eardrum. With the pneumatic otoscope, the doctor gently puffs air against the eardrum. Normally, this puff of air would cause the eardrum to move. If the middle ear is filled with fluid, your doctor will observe little to no movement of the eardrum.
Your doctor may perform other diagnostic tests if there is any doubt about a diagnosis, if the condition hasn't responded to previous treatments, or if there are other persistent or serious problems.
Middle ear infections are caused by bacteria and viruses.
Swelling from an upper respiratory infection or allergy can block theeustachian tubes, which connect the middle ears to the throat. So air can't reach the middle ear. This creates a vacuum and suction, which pulls fluid and germs from the nose and throat into the middle ear. The swollen tube prevents this fluid from draining. The fluid is a perfect breeding ground for bacteria or viruses to grow into an ear infection.
Inflammation and fluid buildup can occur without infection and cause a feeling of stuffiness in the ears. This is known as otitis media with effusion.
Symptoms of a middle ear infection (acute otitis media) often start 2 to 7 days after the start of a cold or other upper respiratory infection. Symptoms of an ear infection may include:
The Eustachian tube runs from the middle of each ear to the back of the throat. This tube drains fluid made in the middle ear. If the Eustachian tube becomes blocked, fluid can build up. When this happens, infection can occur. A chronic ear infection develops when fluid or an infection behind the eardrum does not go away.

A chronic ear infection may be caused by:

"Suppurative chronic otitis" is a phrase health care providers use to describe an eardrum that keeps rupturing, draining, or swelling in the middle ear or mastoid area and does not go away.
Ear infections are more common in children because their Eustachian tubes are shorter, narrower, and more horizontal than in adults. Chronic ear infections are much less common than acute ear infections.
Symptoms of a chronic ear infection may be less severe than symptoms of an acute infection. The problem may go unnoticed and untreated for a long time.
Symptoms may include:
Symptoms may continue or come and go. They may occur in one or both ears.
The health care provider will examine the ears. This may reveal:
Tests may include:
Ear infections can be chronic or acute. Acute ear infections are painful but short in duration. Chronic ear infections do not clear up, or they recur many times. Chronic ear infections can cause permanent damage to the middle and inner ear
.
The first treatment of a middle ear infection focuses on relieving pain. The doctor will also assess your child for any risk of complications.
If your child's condition improves in the first couple of days, treating the symptoms at home may be all that is needed. For more information, seeHome Treatment.
If your child isn't better after a couple of days of home treatment, call your doctor. He or she may prescribe antibiotics.
Follow-up exams with a doctor are important to check for persistent infection, fluid behind the eardrum (otitis media with effusion), or repeat infections. Even if your child seems well, he or she may need a follow-up visit in about 4 weeks, especially if your child is young.
Your doctor can give your child antibiotics, but ear infections often get better without them. Talk about this with your doctor. Whether you useantibiotics will depend on how old your child is and how bad the infection is. For more information, see Medications.
Antibiotics can treat ear infections caused by bacteria. But most children with ear infections get better without them. If the care you give at home relieves pain and the symptoms are getting better after a few days, you may not need antibiotics.
Your doctor will likely give antibiotics if:1
For children ages 2 and older, many doctors wait for a few days to see if the ear infection will get better on its own. When doctors do prescribe antibiotics, they most often use amoxicillin, because it works well and costs less than other brands.
When your child takes antibiotics for an ear infection, it is very important to take all of the medicine as directed, even if your child feels better. Do not use leftover antibiotics to treat another illness. Misuse of antibiotics can lead to drug-resistant bacteria.
Some doctors prefer to treat all ear infections with antibiotics, because it's hard to tell which ear infections will clear up on their own. Some things to consider before your child takes antibiotics include:
Antibiotics have only minimal benefits in reducing pain and fever.
If your child still has symptoms (fever and earache) longer than 48 hours after starting an antibiotic, a different antibiotic may work better. Call your doctor if your child isn't feeling better after 2 days of antibiotic treatment.
You may be able to prevent your child from getting middle ear infections.

The provider may prescribe antibiotics if the infection is caused by bacteria. These medicines may need to be taken for a long time. They can be given by mouth or into a vein (intravenously).
If there is a hole in the eardrum, antibiotic ear drops are used. The provider may recommend using a mild acidic solution (such as vinegar and water) for a hard-to-treat infected ear that has a hole (perforation). A surgeon may need to clean out (debride) tissue that has gathered inside the ear.
Other surgeries that may be needed include:
Chronic ear infections most often respond to treatment. However, your child may need to keep taking medicines for several months.
Chronic ear infections are not life threatening. However, they can be uncomfortable and may result in hearing loss and other serious complications.
A chronic ear infection may cause permanent changes to the ear and nearby bones, including:
Hearing loss from damage to the middle ear may slow language and speech development. This is more likely if both ears are affected.
Permanent hearing loss is rare, but the risk increases with the number and length of infections.
Call your health care provider if:
Getting prompt treatment for an acute ear infection may reduce the risk of developing a chronic ear infection. Have a follow-up exam with your provider after an ear infection has been treated to make sure that it is completely cured.