
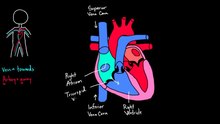
Aorta
the body's largest artery. Takes oxygenated blood from the left ventricle to the body.

The heart is a muscular organ about the size of a fist, located just behind and slightly left of the breastbone. The heart pumps blood through the network of arteries and veins called the cardiovascular system.
The heart has four chambers:
The coronary arteries run along the surface of the heart and provide oxygen-rich blood to the heart muscle. A web of nerve tissue also runs through the heart, conducting the complex signals that govern contraction and relaxation. Surrounding the heart is a sac called the pericardium.

The heart is situated in the middle mediastinum behind the breastbone in the chest, at the level of thoracic vertebrae T5-T8. The largest part of the heart is usually slightly offset to the left side of the chest (though occasionally it may be offset to the right) and is felt to be on the left because the left heart is stronger, since it pumps to all body parts. Because the heart is between the lungs, the left lung is smaller than the right lung and has a cardiac notch in its border to accommodate the heart.
The heart is supplied by the coronary circulation and is enclosed in a double-membraned sac–the pericardium. This attaches to the mediastinum, providing anchorage for the heart.[15] The back surface of the heart lies near to the vertebral column, and the front surface sits deep to the sternum and costal cartilages.[7] Two of the great veins – the venae cavae, and the great arteries, the aorta and pulmonary artery, are attached to the upper part of the heart, called the base, which is located at the level of the third costal cartilage.[7] The lower tip of the heart, the apex, lies to the left of the sternum (8 to 9 cm from the midsternal line) between the junction of the fourth and fifth ribs near their articulation with the costal cartilages.[7] The right side of the heart is deflected forwards, and the left deflected to the back.[7]
The heart is cone-shaped, with its base positioned upwards and tapering down to the apex.[7] A stethoscope can be placed directly over the apex so that the heartbeats can be counted. An adult heart has a mass of 250–350 grams (9–12 oz).[16] The heart is typically the size of a fist: 12 cm (5 in) in length, 8 cm (3.5 in) wide, and 6 cm (2.5 in) in thickness.[7] Well-trained athletes can have much larger hearts due to the effects of exercise on the heart muscle, similar to the response of skeletal muscle.[7]

The heart wall is made up of three layers: the inner endocardium, middle myocardium and outer epicardium. These are surrounded by a double-membraned sac called the pericardium.
The innermost layer of the heart is called the endocardium. It is made up of a lining of simple squamous epithelium, and covers heart chambers and valves. It is continuous with the endothelium of the veins and arteries of the heart, and is joined to the myocardium with a thin layer of connective tissue.[7] The endocardium, by secreting endothelins, may also play a role in regulating the contraction of the myocardium.[7]

The middle layer of the heart wall is the myocardium, which is the cardiac muscle– a layer of involuntary striated muscle tissue surrounded by a framework ofcollagen. The myocardium is also supplied with blood vessels, and nerve fibers by way of the epicardium that help to regulate the heart rate.[7] Cardiac muscle tissue has autorhythmicity, the unique ability to initiate a cardiac action potential at a fixed rate – spreading the impulse rapidly from cell to cell to trigger thecontraction of the entire heart. This autorhythmicity is still modulated by the endocrine and nervous systems.[7]
There are two types of cardiac muscle cell: cardiomyocytes which have the ability to contract easily, and modified cardiomyocytes the pacemaker cells of the conducting system. The cardiomyocytes make up the bulk (99%) of cells in the atria and ventricles. These contractile cells are connected by intercalated discs which allow a rapid response to impulses of action potential from the pacemaker cells. The intercalated discs allow the cells to act as a syncytium and enable the contractions that pump blood through the heart and into the major arteries.[7]
The pacemaker cells make up 1% of cells and form the conduction system of the heart. They are generally much smaller than the contractile cells and have fewmyofibrils which gives them limited contractibility. Their function is similar in many respects to neurons.[7]
The cardiac muscle pattern is elegant and complex, as the muscle cells swirl and spiral around the chambers of the heart.[7] They form a figure 8 pattern around the atria and around the bases of the great vessels.[7] Deeper ventricular muscles also form a figure 8 around the two ventricles and proceed toward the apex. More superficial layers of ventricular muscle wrap around both ventricles.[7] This complex swirling pattern allows the heart to pump blood more effectively than a simple linear pattern would.[7]
As with skeletal muscles the heart can increase in size and efficiency with exercise.[7] Thus endurance athletes such as marathon runners may have a heart that hasincreased in size by up to 40%.[17]
The pericardium surrounds the heart. It consists of two membranes: an inner serous membrane called the epicardium, and an outer fibrous membrane. These enclose the pericardial cavity which contains the pericardial fluid that lubricates the surface of the heart.[18]

The heart has four chambers, two upper atria, the receiving chambers, and two lower ventricles, the discharging chambers. The atria open into the ventricles via the atrioventricular valves, present in the atrioventricular septum. This distinction is visible also on the surface of the heart as the coronary sulcus.[19] There is an ear-shaped structure in the upper right atrium called the right atrial appendage, or auricle, and another in the upper left atrium, the left atrial appendage.[20] The right atrium and the right ventricle together are sometimes referred to as the right heart. Similarly, the left atrium and the left ventricle together are sometimes referred to as the left heart.[6] The ventricles are separated from each other by the interventricular septum, visible on the surface of the heart as the anterior longitudinal sulcusand the posterior interventricular sulcus.[19]
The cardiac skeleton is made of dense connective tissue and this gives structure to the heart. It forms the atrioventricular septum which separates the atria from the ventricles, and the fibrous rings which serve as bases for the four heart valves.[21] The cardiac skeleton also provides an important boundary in the heart's electrical conduction system since collagen cannot conduct electricity. The interatrial septum separates the atria and the interventricular septum separates the ventricles.[7] The interventricular septum is much thicker than the interatrial septum, since the ventricles need to generate greater pressure when they contract.[7]

.svg)

The heart has four valves, which separate its chambers.[7] The valves ensure blood flows in the correct direction through the heart and prevents backflow. Between the right atrium and the right ventricle is the tricuspid valve. This consists of three cusps (flaps or leaflets), made of endocardium reinforced with additional connective tissue. Each of the three valve-cusps is attached to several strands of connective tissue, the chordae tendineae (tendinous cords).[22] They are composed of approximately 80 percentcollagenous fibers with the remainder consisting of elastic fibers and endothelium.[citation needed] They connect each of the cusps to apapillary muscle that extends from the walls of the ventricle. These muscles prevent the valve from falling back into the atrium.[23][g] The three papillary muscles in the right ventricle are called the anterior, posterior, and septal muscles, which correspond to the three positions of the valve cusps.[22]
Between the left atrium and left ventricle is the mitral valve, also known as the bicuspid valve due to its having two cusps, an anterior and a posterior cusp. These cusps are also attached via chordae tendinae to two papillary muscles projecting from the ventricular wall.[24]
The tricuspid and the mitral valves are the atrioventricular valves. During the relaxation phase of the cardiac cycle, the papillary muscles are also relaxed and the tension on the chordae tendineae is slight. However, as the ventricle contracts, so do the papillary muscles. This creates tension on the chordae tendineae, helping to hold the cusps of the atrioventricular valves in place and preventing them from being blown back into the atria.[7]
The semilunar pulmonary valve is located at the base of the pulmonary artery. This has three cusps which are not attached to any papillary muscles. When the ventricle relaxes blood flows back into the ventricle from the artery and this flow of blood fills the pocket-like valve, pressing against the cusps which close to seal the valve. The semilunar aortic valve is at the base of the aorta and also is not attached to papillary muscles. This too has three cusps which close with the pressure of the blood flowing back from the aorta.[7]
The two major systemic veins, the superior and inferior venae cavae, and the collection of veins that make up the coronary sinus which drains the myocardium, empty into the right atrium. The superior vena cava drains blood from above the diaphragm and empties into the upper back part of the right atrium. The inferior vena cava drains the blood from below the diaphragm and empties into the back part of the atrium below the opening for the superior vena cava. Immediately above and to the middle of the opening of the inferior vena cava is the opening of the thin-walled coronary sinus.[7]
In the wall of the right atrium is an oval-shaped depression known as the fossa ovalis, which is a remnant of an opening in the fetal heart known as the foramen ovale. The foramen ovale allowed blood in the fetal heart to pass directly from the right atrium to the left atrium, allowing some blood to bypass the pulmonary circuit. Within seconds after birth, a flap of tissue known as the septum primum that previously acted as a valve closes the foramen ovale and establishes the typical cardiac circulation pattern.[7] Most of the internal surface of the right atrium is smooth, the depression of the fossa ovalis is medial, and the anterior surface has prominent ridges of pectinate muscles, which are also present in the right atrial appendage.[7]
The atria receive venous blood on a nearly continuous basis, preventing venous flow from stopping while the ventricles are contracting. While most ventricular filling occurs while the atria are relaxed, they do demonstrate a contractile phase when they actively pump blood into the ventricles just prior to ventricular contraction. The right atrium is connected to the right ventricle by the tricuspid valve.[7]
When the myocardium of the ventricle contracts, pressure within the ventricular chamber rises. Blood, like any fluid, flows from higher pressure to lower pressure areas, in this case, toward the pulmonary artery and the atrium. To prevent any potential backflow, the papillary muscles also contract, generating tension on the chordae tendineae. This prevents the flaps of the valves from being forced into the atria and regurgitation of the blood back into the atria during ventricular contraction.[7]
The walls of the right ventricle are lined with trabeculae carneae, ridges of cardiac muscle covered by endocardium. In addition to these muscular ridges, a band of cardiac muscle, also covered by endocardium, known as the moderator band reinforces the thin walls of the right ventricle and plays a crucial role in cardiac conduction. It arises from the lower part of the interventricular septum and crosses the interior space of the right ventricle to connect with the inferior papillary muscle.[7]
When the right ventricle contracts, it ejects blood into the pulmonary artery, which branches into the left and right pulmonary arteries that carry it to each lung. The upper surface of the right ventricle begins to taper as it approaches the pulmonary artery. At the base of the pulmonary artery is the pulmonary semilunar valve that prevents backflow from the pulmonary artery.[7]
After gas exchange in the pulmonary capillaries, blood high in oxygen returns to the left atrium via one of the four pulmonary veins. Only the left atrial appendage contains pectinate muscles. Blood flows nearly continuously from the pulmonary veins back into the atrium, which acts as the receiving chamber, and from here through an opening into the left ventricle. Most blood flows passively into the heart while both the atria and ventricles are relaxed, but toward the end of the ventricular relaxation period, the left atrium will contract, pumping blood into the ventricle. This atrial contraction accounts for approximately 20 percent of ventricular filling. The left atrium is connected to the left ventricle by the mitral valve.[7]
Although both sides of the heart will pump the same amount of blood, the muscular layer is much thicker in the left ventricle compared to the right, due to the greater force needed here. Like the right ventricle, the left also has trabeculae carneae, but there is no moderator band. The left ventricle is the major pumping chamber for the systemic circuit; it ejects blood into the aorta through the aortic semilunar valve.[7]

Coronary arteries supply oxygen-rich blood to the heart and the coronary veins remove the deoxygenated blood. There is a left and a right coronary arterysupplying the left and right hearts respectively, and the septa. Smaller branches of these arteries anastomose, which in other parts of the body serve to divert blood due to a blockage. In the heart these are very small and cannot form other interconnections with the result that a coronary artery blockage can cause amyocardial infarction and with it, tissue damage.[7]
The great cardiac vein receives the major branches of the posterior, middle, and small cardiac veins and drains into the coronary sinus, a large vein that empties into the right atrium. The anterior cardiac veins drain the front of the right ventricle and drain directly into the right atrium.[7]


The heart is the first functional organ to develop and starts to beat and pump blood at about three weeks into embryogenesis. This early start is crucial for subsequent embryonic andprenatal development.
The heart derives from splanchnopleuric mesenchyme in the neural plate which forms the cardiogenic region. Two endocardial tubes form here that fuse to form a primitive heart tube known as the tubular heart.[25] Between the third and fourth week, the heart tube lengthens, and begins to fold to form an S-shape within the pericardium. This places the chambers and major vessels into the correct alignment for the developed heart. Further development will include the septa and valves formation and remodelling of the heart chambers. By the end of the fifth week the septa are complete and the heart valves are completed by the ninth week.[7]
The embryonic heart begins beating at around 22 days after conception (5 weeks after the last normal menstrual period, LMP). It starts to beat at a rate near to the mother's which is about 75–80 beats per minute (bpm). The embryonic heart rate then accelerates and reaches a peak rate of 165–185 bpm early in the early 7th week (early 9th week after the LMP).[26][27] After 9 weeks (start of the fetal stage) it starts to decelerate, slowing to around 145 (±25) bpm at birth. There is no difference in female and male heart rates before birth.[28]

The heart functions as a pump in the circulatory system to provide a continuous circulation of blood throughout the body. This circulation consists of the systemic circulation to and from the body and the pulmonary circulation to and from the lungs. Blood in the pulmonary circulation exchanges carbon dioxide for oxygen in the lungs through the process ofrespiration. The systemic circulation then transports oxygen to the body and returns carbon dioxide and relatively deoxygenated blood to the heart for transfer to the lungs.[7]
The right heart collects deoxygenated blood from two large veins, the superior and inferior venae cavae. The blood collects in the right atrium and is pumped through the tricuspid valve into the right ventricle, where it is pumped into the pulmonary artery through the pulmonary valve. Here the blood enters the pulmonary circulation where carbon dioxide can be exchangedfor oxygen in the lungs. This happens through the passive process of diffusion.
In the left heart, oxygenated blood is returned to the left atrium via the pulmonary veins. It is then pumped into the left ventricle through the mitral valve and into the aorta through the aortic valve for systemic circulation. The aorta is a large artery that branches into many smaller arteries, arterioles, and ultimately capillaries. In the capillaries, oxygen and nutrients from blood are supplied to body cells for metabolism, and exchanged for carbon dioxide and waste products[7]


The cardiac cycle refers to a complete heartbeat which includes systole and diastole and the intervening pause.[9] The cycle begins with contraction of the atria and ends with relaxation of the ventricles. Systole is when the ventricles of the heart contract to pump blood to the body. Diastole is when the ventricles relax and fill with blood. The atria and ventricles work in concert, so in systole when the ventricles are contracting, the atria are relaxed and collecting blood. When the ventricles are relaxed in diastole, the atria contract to pump blood to the ventricles. This coordination ensures blood is pumped efficiently to the body.[7]
At the beginning of the cardiac cycle, in early diastole, both the atria and ventricles are relaxed. Since blood moves from areas of high pressure to areas of low pressure, when the chambers are relaxed, blood will flow into the atria (through the coronary sinus and the pulmonary veins). As the atria begin to fill, the pressure will rise so that the blood will move from the atria into the ventricles. In late diastole the atria contract pumping more blood into the ventricles. This causes a rise in pressure in the ventricles, and in ventricular systole blood will be pumped into the pulmonary artery.[9]
When the atrioventricular valves (tricuspid and mitral) are open, during blood flow to the ventricles, the semilunar valves are closed to prevent backflow into the ventricles. When the ventricular pressure is greater than the atrial pressure the tricuspid and mitral valves will shut. When the ventricles contract the pressure forces the semilunar aortic and pulmonary valves open. As the ventricles relax the semilunar valves will close in response to decreased pressure.[9]

Cardiac output (CO) is a measurement of the amount of blood pumped by each ventricle (stroke volume) in one minute. This is calculated by multiplying the stroke volume (SV) by the beats per minute of the heart rate (HR). So that: CO = SV x HR.[7]
The average cardiac output, using an average SV of about 70mL, is 5.25 L/min, with a range of 4.0–8.0 L/min.[7] The stroke volume is normally measured using anechocardiogram and can be influenced by the size of the heart, physical and mental condition of the individual, sex, contractility, duration of contraction, preloadand afterload.[7]
Preload refers to the filling pressure of the atria at the end of diastole, when they are at their fullest. A main factor is how long it takes the ventricles to fill—if the ventricles contract faster, then there is less time to fill and the preload will be less.[7] Preload can also be affected by a person's hydration status. The force of each contraction of the heart muscle is proportional to the preload, described as the Frank-Starling mechanism. This states that the force of contraction is directly proportional to the initial length of muscle fiber, meaning a ventricle will contract more forcefully, the more it is stretched.[7][29]
Afterload, or how much pressure the heart must generate to eject blood at systole, is influenced by vascular resistance. It can be influenced by narrowing of the heart valves (stenosis) or contraction or relaxation of the peripheral blood vessels.[7]
The strength of heart muscle contractions controls the stroke volume. This can be influenced positively or negatively by agents termed inotropes. These can be either conditions or drugs. Positive inotropes that cause stronger contractions include high blood calcium and drugs such as Digoxin, which will act to stimulate thesympathetic nerves in the fight-or-flight response. Negative inotropes causing weaker contractions include high blood potassium, hypoxia, acidosis, and drugs such as beta blockers and calcium channel blockers.

The normal rhythmical heart beat, called sinus rhythm, is established by the sinoatrial node, the heart's pacemaker. Here an electrical signal is created that travels through the heart, causing the heart muscle to contract.
The sinoatrial node is found in the upper part of the right atrium near to the junction with the superior vena cava.[30] The electrical signal generated by the sinoatrial node travels through the right atrium in a radial way that is not completely understood. It travels to the left atrium via Bachmann's bundle, such that both left and right atria contract together.[31][32][33] The signal then travels to the atrioventricular node. This is found at the bottom of the right atrium in the atrioventricular septum—the boundary between the right atrium and the left ventricle. The septum is part of the cardiac skeleton, tissue within the heart that the electrical signal cannot pass through, which forces the signal to pass through the atrioventricular node only.[7] The signal then travels along the Bundle of His to left and rightbundle branches through to the ventricles of the heart. In the ventricles the signal is carried by specialized tissue called the Purkinje fibers which then transmit the electric charge to the cardiac muscle.[34]


The sinoatrial node creates and sustains its own rhythm, the sinus rhythm. Cells in the sinoatrial node do this by creating an action potential. The cardiac action potential is created by the movement of specific electrolytes into and out of the pacemaker cells. The action potential then spreads to nearby cells.[35]
When the sinoatrial cells are resting, they have a negative charge on their membranes. However a rapid influx of sodium ions causes the membrane's charge to become positive. This is called depolarisation and occurs spontaneously.[7] Once the cell has a sufficiently high charge, the sodium channels close and calcium ions then begin to enter the cell, shortly after which potassium begins to leave it. All the ions travel through ion channels in the membrane of the sinoatrial cells. The potassium and calcium only start to move out of and into the cell once it has a sufficiently high charge, and so are called voltage-gated. Shortly after this, the calcium channels close and potassium channels open, allowing potassium to leave the cell. This causes the cell to have a negative resting charge and is called repolarization. When the membrane potential reaches approximately ?60 mV, the potassium channels close and the process may begin again.[7]
The ions move from areas where they are concentrated to where they are not. For this reason sodium moves into the cell from outside, and potassium moves from within the cell to outside the cell. Calcium also plays a critical role. Their influx through slow channels means that the sinoatrial cells have a prolonged "plateau" phase when they have a positive charge. A part of this is called the absolute refractory period. Calcium ions also combine with the regulatory protein troponin C in the troponin complex to enable contraction of the cardiac muscle, and separate from the protein to allow relaxation.[36]

The normal sinus rhythm of the heart, giving the resting heart rate, is influenced by the autonomic nervous system through sympathetic andparasympathetic nerves.[37] These arise from two paired cardiovascular centres in the medulla oblongata.The vagus nerve of the parasympathetic nervous system acts to decrease the heart rate, and nerves from the sympathetic trunk act to increase the heart rate. These come together in the cardiac plexusnear the base of the heart. Without parasympathetic input which normally predominates, the sinoatrial node would generate a heart rate of about 100 bpm.[7]
The nerves from the sympathetic trunk emerge through the T1-T4 thoracic ganglia and travel to both the sinoatrial and atrioventricular nodes, as well as to the atria and ventricles. The ventricles are more richly innervated by sympathetic fibers than parasympathetic fibers. Sympathetic stimulation causes the release of the neurotransmitter norepinephrine (also known as noradrenaline) at the neuromuscular junction of the cardiac nerves. This shortens the repolarization period, thus speeding the rate of depolarization and contraction, which results in an increased heart rate. It opens chemical or ligand-gated sodium and calcium ion channels, allowing an influx of positively charged ions.[7] Norepinephrine binds to the beta–1 receptor. High blood pressure medications are used to block these receptors and so reduce the heart rate.[7]
The cardiovascular centres receive input from a series of receptors including proprioreceptors, baroreceptors, and chemoreceptors, plus stimuli from the limbic system. Through a series of reflexes these help regulate and sustain blood flow. For example, increased physical activity results in increased rates of firing by various proprioreceptors located in muscles, joint capsules, and tendons. With increased rates of firing, the parasympathetic stimulation may decrease or sympathetic stimulation may increase as needed in order to increase blood flow.[7]
Similarly, baroreceptors are stretch receptors located in the aortic sinus, carotid bodies, the venae cavae, and other locations, including pulmonary vessels and the right side of the heart itself. Rates of firing from the baroreceptors represent blood pressure, level of physical activity, and the relative distribution of blood. The cardiac centers monitor baroreceptor firing to maintain cardiac homeostasis, a mechanism called the baroreceptor reflex. With increased pressure and stretch, the rate of baroreceptor firing increases, and the cardiac centers decrease sympathetic stimulation and increase parasympathetic stimulation. As pressure and stretch decrease, the rate of baroreceptor firing decreases, and the cardiac centers increase sympathetic stimulation and decrease parasympathetic stimulation.[7]
There is a similar reflex, called the atrial reflex or Bainbridge reflex, associated with varying rates of blood flow to the atria. Increased venous return stretches the walls of the atria where specialized baroreceptors are located. However, as the atrial baroreceptors increase their rate of firing and as they stretch due to the increased blood pressure, the cardiac center responds by increasing sympathetic stimulation and inhibiting parasympathetic stimulation to increase HR. The opposite is also true.[7]
In addition to the autonomic nervous system, other factors can impact on this. These include epinephrine, norepinephrine, and thyroid hormones; levels of various ions including calcium, potassium, and sodium; body temperature; hypoxia; and pH balance. Factors that increase the heart rate can include release ofnorepinephrine, hypoxemia, low blood pressure and dehydration, a strong emotional response, a higher body temperature, and metabolic and hormonal factors such as a low potassium or sodium level or stimulus from thyroid hormones.[7] Decreased body temperature, relaxation, and metabolic factors can also contribute to a decrease in heart rate.[7]
The resting heart rate of a newborn can be 129 beats per minute (bpm) and this gradually decreases until maturity.[38] The adult resting heart rate ranges from 60 to 100 bpm. Exercise and fitness levels, age and basal metabolic rate can all affect the heart rate. An athlete's heart rate can be lower than 60 bpm. During exercise the rate can be 150 bpm with maximum rates reaching from 200 to 220 bpm.[7]

Heart murmurs are abnormal heart sounds which can be either pathological or benign.[40] One example of a murmur is Still's murmur, which presents a musical sound in children, has no symptoms and disappears in adolescence.[41]
A different type of sound, a pericardial friction rub can be heard in cases of pericarditis where the inflamed membranes can rub together.[42]


Cardiovascular diseases, which include diseases of the heart, are the leading cause of death worldwide.[43] The majority of cardiovascular disease is noncommunicable and related to lifestyle and other factors, becoming more prevalent with ageing.[43] Heart disease is a major cause of death, accounting for an average of 30% of all deaths in 2008, globally.[11] This rate varies from a lower 28% to a high 40% in high-income countries.[12] Doctors that specialise in the heart are called cardiologists. Many other medical professionals are involved in treating diseases of the heart, including doctors such as general practitioners,cardiothoracic surgeons and intensivists, and allied health practitioners including physiotherapists and dieticians.[44]
Coronary artery disease is also known as ischemic heart disease, is caused by atherosclerosis – a build-up of plaque along the inner walls of the arteries whichnarrows them, reducing the blood flow to the heart.[45] A stable plaque may cause chest pain (angina) or breathlessness during exercise or at rest, or no symptoms at all. A ruptured plaque can block a blood vessel and lead to ischaemia of the heart muscle, causing unstable angina or a heart attack.[46] In the worst case this may cause cardiac arrest, a sudden and utter loss of output from the heart.[47] Obesity, high blood pressure, uncontrolled diabetes, smoking and high cholesterolcan all increase the risk of developing atherosclerosis and coronary artery disease.[43][45]
Heart failure is where the heart can't beat enough blood to meet the needs of the body.[45] It is generally a chronic condition, associated with age, that progresses gradually.[48]Each side of the heart can fail independently of the other, resulting in heart failure of the right heart or the left heart. Left heart failure can also lead to right heart failure by increasing strain on the right heart (called cor pulmonale). If the heart is unable to pump sufficient blood, it may accumulate throughout the body, causing breathlessness in the lungs (pulmonary congestion; pulmonary edema), swelling (edema) of the feet or other gravity-dependent areas, decrease exercise tolerance, or cause other clinical signs such as an enlarged liver, cardiac murmurs, or a raised jugular venous pressure. Common causes of heart failure include coronary artery disease, valve disorders and diseases of cardiac muscle.[49]
Cardiomyopathy is a noticeable deterioration of the heart muscle's ability to contract, which can lead to heart failure. The causes of many types cardiomyopathy are poorly understood; some identified causes include alcohol, toxins, systemic disease such as sarcoidosis, and congenital conditions such as HOCM. The types of cardiomyopathy are described according to how they affect heart muscle. Cardiomyopathy can cause the heart to become enlarged (hypertrophic cardiomyopathy), constrict the outflow tracts of the heart (restrictive cardiomyopathy), or cause the heart to dilate and impact on the effiency of its beating (dilated cardiomyopathy).[50] HOCM is often undiagnosed and can cause sudden death in young athletes.[7]
Heart murmurs are abnormal heart sounds which can be either related to disease or benign, and there are several kinds.[51] There are normally two heart sounds, and abnormal heart sounds can either be extra sounds, or "murmurs" related to the flow of blood between the sounds. Murmurs are graded by volume, from 1) the quietest, to 6) the loudest, and evaluated by their relationship to the heart sounds, position in the cardiac cycle, and additional features such as their radiation to other sites, changes with a person's position, the frequency of the sound as determined by the side of the stethoscope by which they are heard, and site at which they are heard loudest.[51]Phonocardiograms can record these sounds,[7] and echocardiograms are generally required for their diagnosis.[51] Murmurs can result from valvular heart diseases due to narrowing (stenosis), or regurgitation of any of the main heart valves, such as aortic stenosis, mitral regurgitation or mitral valve prolapse. They can also result from a number of other disorders, including atrial and ventricular septal defects.[51] Two common and infective causes of heart murmurs, are infective endocarditis and rheumatic fever, particularly in developing countries. Infective endocarditis involves colonisation of a heart valve,[52] and rheumatic fever involves an initial bacterial infection by Group A streptococcus followed by a reaction against heart tissue that resembles the streptococcal antigen.[53]
Abnormalities in the normal sinus rhythm of the heart can prevent the heart from effectively pumping blood, and are generally identified by ECG. These cardiac arrhythmias can cause an abnormal but regular heart rhythm, such as a rapid heart rate (tachycardia, classified as arising from above the ventricles or from the ventricles) or a slow heart rate (bradycardia); or may result in irregular rhythms. Tachycardia is generally defined as a heart rate faster than 100 beats per minute, and bradycardia as a heart rate slower than 60.[54] Asystole is the cessation of heart rhythm. An irregular rhythm is classified as atrial or ventricular fibrillation depending if the electrical activity originates in the atria or the ventricles.[54] Abnormal conduction can cause a delay or unusual order of contraction of the heart muscle. This can be a result of a disease process, such as heart block, or congenital, such as Wolff-Parkinson-White syndrome.[54]
Diseases may also affect the pericardium which surrounds the heart, which when inflammed is called pericarditis. This may result from infective causes (such as glandular fever, cytomegalovirus,coxsackievirus, tuberculosis or Q fever), systemic disorders such as amyloidosis or sarcoidosis, tumours, high uric acid levels, and other causes. This inflammation affects the ability of the heart to pump effectively. When fluid builds up in the pericardium this is called pericardial effusion, which when it causes acute heart failure is called cardiac tamponade. This may be blood from a traumatic injury or fluid from an effusion.[55] This can compress the heart and adversely affect the function of the heart. The fluid can be removed from the pericardial sac using a syringe in a procedure calledpericardiocentesis.[56]
The heart can be affected by congenital diseases. These include failure of the developmental foramen ovale to close, present in up to 25% of people;[57] ventricular or atrial septal defects, congenital diseases of the heart valves (e.g. congenital aortic stenosis) or disease relating to blood vessels or blood flow from the heart (such as a patent ductus arteriosus or aortic coarctation).;[58] Harrisons 1458–1465 These may cause symptoms at a variety of ages. If unoxygenated blood travels directly from the right to the left side of the heart, it may be noticed at birth, as it may cause a baby to become blue (cyanotic) such as Tetralogy of Fallot. A heart problem may impact a child's ability to grow.[58] Some causes rectify with time and are regarded as benign. Other causes may be incidentally detected on a cardiac examination. These disorders are often diagnosed on an echocardiogram.[59]
Heart disease is diagnosed by the taking of a medical history, a cardiac examination, and further investigations, including blood tests, echocardiograms, ECGs and imaging. Other invasive procedures such as cardiac catheterisation can also play a role.[60]

Using surface electrodes on the body, it is possible to record the complex electrical activity of the heart. This tracing of the electrical signal is the electrocardiogram (ECG) or (EKG). An ECG is a bedside test and usually requires the placement of nine leads on the body. This produces a "12 lead" ECG (three extra leads are calculated mathematically).[62]
There are five prominent points on the ECG: the P wave (atrial depolarisation), the QRS complex (atrial repolarisation and ventricular depolarisation) and the T wave (ventricular repolarisation).[7] These reflect the summed action potential of cardiac myocytes as they contract. A downward deflection on the ECG implies cells are becoming more negative in charge ("depolarising"), whereas an upward inflection implies cells are becoming more positive ("repolarising"). The ECG is a useful tool in detecting rhythm disturbances and in detecting insufficient blood supply to the heart.[61] Sometimes abnormalities are not immediately visible on the ECG. Testing when exercising can be used to provoke an abnormality, or an ECG can be worn for a longer period such as a 24-hour Holter monitor if a rhythm abnormality is suspected to be present but not present at the time of assessment The heart is a muscular organ in both humans and other animals, which pumps blood through the blood vessels of the circulatory system. Blood provides the body with oxygen and nutrients, and also assists in the removal of metabolic wastes.
Note:
The physical form and structure of the heart is shown and described on the page about The Structure of the Heart
The following diagrams are simple summaries of the main parts of the heart, the functions of which are described below.
The main functions of the heart can be summarised as follows:
Right-Hand Side of the Heart The right-hand side of the heart receives de-oxygenated blood from the body tissues (from the upper- and lower-body via thesuperior vena cava and the inferior vena cava, respectively) into the right atrium. This de-oxygenated blood passes through thetricuspid valve into the right ventricle. This blood is then pumped under higher pressure from the right ventricle to the lungs via the pulmonary artery. | Left-Hand Side of the Heart The left-hand side of the heart receives oxygenated blood from the lungs (via the pulmonary veins) into the left atrium. This oxygenated blood then passes through the bicuspid valve into the left ventricle. It is then pumped to the aorta under greater pressure (as explained below). This higher pressure ensures that the oxygenated blood leaving the heart via the aorta is effectively delivered to other parts of the body via the vascular system of blood vessels (incl. arteries, arterioles, andcapillaries). |
the body's largest artery. Takes oxygenated blood from the left ventricle to the body.
Heart disease describes a range of conditions that affect your heart. Diseases under the heart disease umbrella include blood vessel diseases, such as coronary artery disease; heart rhythm problems (arrhythmias); and heart defects you're born with (congenital heart defects), among others.
The term "heart disease" is often used interchangeably with the term "cardiovascular disease." Cardiovascular disease generally refers to conditions that involve narrowed or blocked blood vessels that can lead to a heart attack, chest pain (angina) or stroke. Other heart conditions, such as those that affect your heart's muscle, valves or rhythm, also are considered forms of heart disease.
Many forms of heart disease can be prevented or treated with healthy lifestyle choices